
Smartphone-based application for EMA assessment of awake bruxism: compliance evaluation in a sample of healthy young adults
ABSTRACT
Objective A smartphone-based ecological momentary assessment (EMA) strategy to collect real time data on awake bruxism (AB) has been recently introduced. The aim of this study was to assess the compliance with its use over 1 week in a sample of healthy young adults.
Method Sixty (N = 60) healthy young adults (mean age 24.2 ± 4.1 years) used a dedicated smartphone application that sent 20 alerts at random times throughout the day. Upon alert receipt, the subjects had to report in real time their condition among five possible options: relaxed jaw muscles, teeth contact, teeth clenching, teeth grinding, and mandible bracing. Compliance rate with the app was assessed at the individual and group level in terms of percentage of answered alerts as well as number of days that were needed to reach the targeted observation period of 7 days with a compliance of at least 60%.
Results The mean compliance recorded with the smartphone application was 67.8% of the total alerts. On average, 9.8 ± 3.2 days (range 7–19) have been necessary to achieve the targeted goal of 7 days with a minimum of 60% alerts/day. No gender differences were detected in any compliance data. Response rate was not different during weekdays or weekends.
Conclusions This investigation is the first attempt to assess individual compliance with EMA for reporting awake bruxism. Results suggest that a smartphone-based strategy can have interesting potential. The compliance rate reported in this study will serve as a comparison standpoint for future investigations.
Clinical significance Based on the recent multidisciplinary focus on the study of awake bruxism, EMA has emerged as a potential approach for use in the clinical and research settings. This investigation suggests that compliance with such strategy is good, thus making it worthy of adoption for the assessment of AB and its clinical implications.
There are additional resources available to enhance your understanding of the topic of bruxism assessment in our Online congress on evidence-based temporomandibular disorders and bruxism treatment.
INTRODUCTION
Bruxism is an oral condition that is gaining increasing attention in several medical fields. Recently, some experts were invited to take part in an International Consensus Meeting that provided separate definitions for sleep bruxism (SB) and awake bruxism (AB) and discussed the possible development and refinement of the available diagnostic strategies [1]. They suggested a diagnostic grading to assess both sleep and awake bruxism as Bpossible,^ Bprobable,^ and Bdefinite.^ In particular, since bruxism has to be considered a jaw-muscle behavior in other-wise healthy individuals, it is recommendable that it is measured in its continuum or on-time occurrence of behavior [1, 2]. Until now, most research has focused on sleep bruxism (SB), while knowledge on AB is fragmental. There are few epidemiological data on AB, and findings are not easy to summarize due to the adoption of different assessment strategies [1–4].
Considering that bruxism is as a masticatory muscle activity (MMA), the recommended strategy is to have electromyographic (EMG) recordings of jaw muscles during sleep or wakefulness [2]. Nonetheless, performing an hour-long EMG recording of jaw muscle activity during wakefulness is difficult for technical reasons and for potentially poor patients’ compliance. Thus, the introduction of ecological momentary assessment (EMA) principles to the study of AB, viz., a real time report of behaviors by the patient, emerged as an interesting assessment option [2]. Several studies [5–8], as well as the consensus paper [2], recommended the possible use of EMA strategies to report AB behaviors, since it is a simple method to collect real-time data in the natural environment.
Recently, smartphone-based EMA approaches have been developed in the clinical research setting, to record reports of five specific oral conditions (i.e., relaxed jaw muscles, tooth contact, teeth clenching, teeth grinding, and mandible bracing) that are related to the spectrum of AB activities. A dedicated app has been ideated, which sends alerts at random times during the day. Upon alert receipt, the subject has to focus on his/her current condition and tap on the corresponding display icon [6]. The potential advantages of using this strategy in the clinical and research fields are quite intuitive, and they have been described in a series of publications [5–9]. On the other hand, there are no data available so far on the com- pliance with the application.
Within these premises, this study evaluated the compliance with the use of a smartphone application for the real-time report of AB behaviors in a sample of healthy young adults. The two-fold aim was to (1) assess the actual feasibility of introducing such strategy in the routine evaluation of AB, and (2) set a potential comparison standpoint for future investigations at population level as well as for validation of reports at the individual level.
MATERIALS AND METHODS
The study was performed on a sample of otherwise healthy young adults, who were recruited among the dental students attending the last 3 years of the School of Dentistry at the University of Ferrara, Ferrara, Italy.
The research protocol was approved by the Treviso Hospital’s IRB (code #344-CES-AULSS9). All individuals gave their informed consent in accordance with the Helsinki Declaration and understood that they were free to withdraw from the study at any time.
Exclusion criteria were the presence of temporomandibular disorders (TMD) pain, as screened with the diagnostic criteria for temporomandibular disorders (DC/TMD) guidelines [10], and/or any documented neurological, psychiatric, sleep, or systemic (e.g., rheumatologic, hormonal) diseases.
The study design provided the use of a dedicated smartphone application (BruxApp®, BruxApp team, Pontedera, Italy). All participants received the information on the application and the instructions to use it during dedicated educational sessions. The leading investigator (AC) organized two training sessions for the students, to provide any necessary information about the application. In short, the app sends alerts at random times during the day. The subject must then answer (i.e., EMA) by tapping on the display within 5 min of the alert. Possible answers are related with five different oral conditions that may be exerted at the moment of the alert sound: relaxed jaw muscles, mandible bracing, teeth contact, teeth clenching, teeth grinding. The project coordinator (DM) also recorded an educational video to describe how to recognize the five behaviors (https://www.youtube.com/watch?v=xL79AcnpBCY&t=15s). For any further details on the application, readers are referred to the original publications [5, 6].
The software was programmed to send 20 alerts at random intervals, to limit expectation bias (e.g., the risk that individuals may modify their behaviors based on the alert expectation, if set at predetermined intervals). Recording time was set from 8:00 to 12:30 and from 14:30 to 22:00.
Data were recorded, and three thresholds for minimum compliance (i.e., T1 8 alerts/day [40%]; T2 12 alerts/day [60%]; T3 16 alerts/day [80%]) were arbitrarily chosen to compare the percentage of subjects who responded to the different thresholds during the first 7 days. The app automatically generated one or more additional days until the target of 7 days in which the subjects had to reply to at least 60% of the total alerts (minimum 12 alerts/day) was reached. After the observation period, the software generated an anonymous pre-formatted excel file that participants sent the leading investigator via email.
Compliance was evaluated according to the following parameters:
The average percentage of subjects who responded to at least 40, 60, and 80% of the total alerts in the first 7 days
The average percentage of answered alerts per day
The difference in compliance between weekend and working days
Gender differences
Statistical analysis
The data were stored in a database and all statistical procedures were performed using the Excel software (Microsoft Corporation, Redmond, WA, USA).
A descriptive analysis of each condition was performed. Data were reported as mean values, standard deviation, and 95% confidence intervals. Gender comparison and working vs weekend days comparison for the percentage of answered alerts were performed using Student’s t test.
Analysis of variance (ANOVA) was used to test for significant differences between the three thresholds as for the average percentage of the subjects who answered at least 40, 60, and 80% of the total alerts in the first 7 days of the use of the application. The level of significance was set at p < 0.05.
RESULTS
Of the 65 students attending the final 3 years of the School of Dentistry, 5 were not eligible for the study, because of a history of TMD pain (N = 4), or the presence of systemic rheumatic disease (N = 1). This led to a final sample of 60 participants (25 males, 35 females; mean age 24.2 ± 4.1 years) taking part to the study.
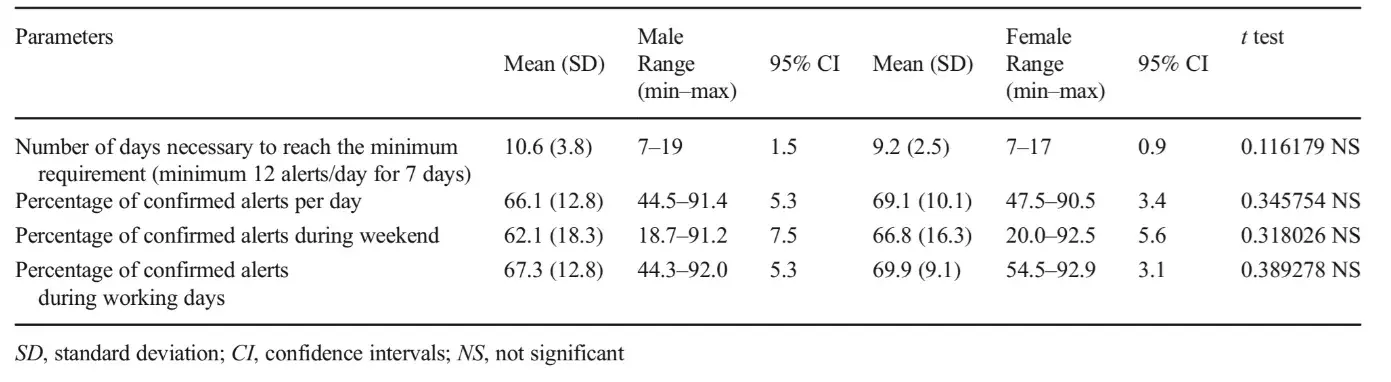
ANOVA showed a statistically significant difference (p < 0.001) between the three thresholds as for the average percentage of subjects who answered at least 40, 60, and 80% of the total alerts: 92.4 ± 3.3% (range 88.3–96.6%), 76.2 ± 10.7% (range 60.0–91.7%), and 28.6 ± 7.9% (range 20.0–38.3%) for a minimum of 8, 12, and 16 alerts/day, respectively (Table 1). The mean compliance per day (i.e., percentage of alerts to which the subjects responded) was 67.8 ± 11.3% (range 44.5–91.4%) of the total alerts. There were no statistically significant differences in the compliance with the use of the app during working days or weekends p = 0.138 (Table 2). Likewise, no differences were found concerning gender comparison in any outcomes, with p values ranging from 0.116 to 0.389 (Table 3).
Assuming the threshold of 12 answered alerts/day (i.e., 60%) as the best compromise between the need to gather as many data as possible and to avoid prolonging too much of the observation period, the mean number of days that were necessary to achieve the target of 7 days was 9.8 ± 3.2 (range 7–19) (Table 2).
Table 1 Descriptive statistics, expressed in percentage, pertaining to the variables (mean value; standard deviation; range) and ANOVA test for significant differences (statistical significance, p < 0.05)
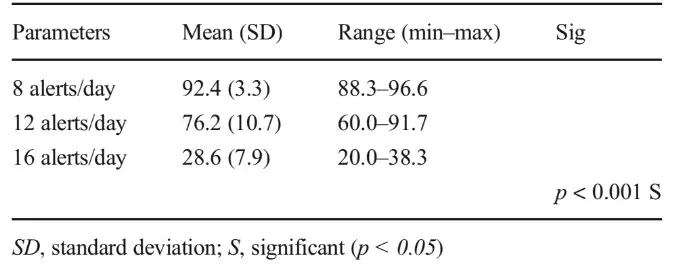
Table 2 Descriptive statistics pertaining to the variables (mean value; standard deviation; range; 95% confidence intervals) and differences between working days vs weekend assessed using Student’s t test (statistical significance p < 0.05)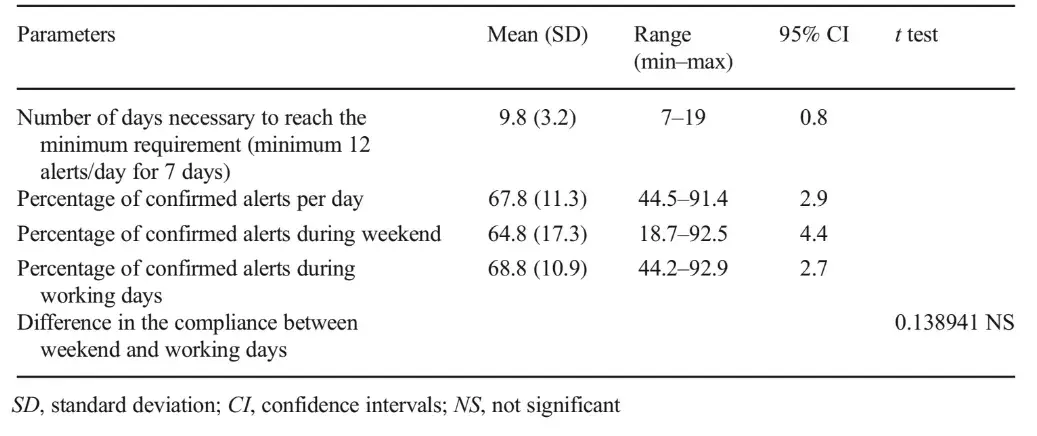
Table 3 Descriptive statistics pertaining to the variables for male and female (mean value; standard deviation; range; 95% confidence intervals) and differences between gender assessed using Student’s t test for each parameter (statistical significance p < 0.05)
DISCUSSION
Knowledge on AB is fragmental [2], due to the difficulties to perform hour-long EMG recordings during wakefulness and the subsequent availability of information that is mainly based on retrospective self-report at a single observation point [4]. Such an approach provides generic answers of doubtful usefulness for the on-field study of the spectrum of AB behaviors, since it requires an individual to recollect the frequency of a Bhabit^ over the timespan covered by the report (e.g., days, weeks, months, and years).
As recently suggested, these limitations can easily be overcome by adopting EMA strategies, which are based on the report of a condition in real time [5–9, 11, 12]. EMA is carried out in natural settings and can be prolonged for several days, thus offering a potential advantage in terms of ecological validity even compared with hour-long EMG recordings during wakefulness. This approach can be optimized with the use of smartphone apps, which are intuitive, easy to use, and only require a simple explanation [13, 14].
Pilot studies using this strategy [5–8] suggested promising developments, but it must be remarked that patients’ compliance has not yet been evaluated. Within these premises, the aim of this study was to assess the compliance with a smartphone-based EMA strategy to collect data on awake bruxism in a sample of healthy, young adults. The clinical implications of this investigation are quite intuitive, concerning the possible validity and standardization of this approach in the clinical and research fields. Findings suggest that compliance levels were good. On average, the participants answered to about two-thirds of the alerts (i.e., 67.8%).
Three different thresholds of answers were assessed: 40% (T1), 60% (T2), 80% (T3). With T1, the average percentage of the subjects who responded in the overall sample was over 90%, compared with T3 where it was less than 30%. Thus, T2 emerged as the best available approach in terms of gathering relevant information (i.e., at least 60% of daily alerts) over a not-too-long time period.
Indeed, with T2, all participants achieved the target of 7 days for which a minimum of 12 alerts/day was required; on average, it took less than 3 extra days to fill the task, which may be understandable because of concurrent daily life duties that may sometimes prevent from answering enough alerts. The most compliant individual took just 7 days, while the longer observation period that was needed to fill the task was 19 days. For comparison purposes, it should be pointed out that these results are similar to studies on the compliance with the use of removable orthodontic devices (i.e., 62%), which are a rare example of comparable investigations in dentistry [15].
Interestingly, no statistically significant differences were found for the compliance during work days or weekends, possibly suggesting that the smartphone-based EMA approach is easy to integrate into a daily routine and that unanswered alerts are due to reasons that are not necessarily related with work or academic duties. This is particularly encouraging if one considers that the protocol [5] adopted in this investigation was quite restrictive: individuals had to tap on the display answering the alert within 5 min, after which, it was not possible to reply (i.e., invalid alert). Findings also showed no gender differences in the compliance, which is also in agreement with investigations on compliance evaluation in other fields, such as orthodontic studies [16–18] assessing the patient’s cooperation in the use of removable devices.
This investigation has a potential shortcoming, viz., the study sample of dentistry students. The possibility that they might have been a stronger motivation and sense of duty than a sample of the general population cannot be excluded. On the other hand, it is plausible that patients who are prescribed with the smartphone-based EMA approach as part of a cognitive-behavioral strategy to manage awake bruxism would exhibit the same level of compliance. As an important clinical implication, a poor compliance with this approach could be indicative of a poor willingness of the patients to be an active part of the AB management regimen, thus representing an unfavorable prognostic factor, as in orthodontics [19]. Poor collaboration might also be related to particular personality features, as in the case of investigations on the compliance of patients to protocols for the management of periodontal disease [20].
Thus, compliance with the use of an app-based EMA could therefore also be interpreted as a potential prognostic factor for the future outcome of bruxism management that should be evaluated with future investigations.
The good compliance reported in this investigation suggests that this approach could be used to study the frequency of conditions of the AB behavioral spectrum in the natural environment (i.e., tooth contact habits, tooth clenching, tooth grinding, and mandible bracing).
Future developments of this strategy encompass the possible identification of a range of Bnormal values^ for AB in healthy individuals for comparison with selected groups of subjects who have associated conditions that may increase bruxism (e.g., stress sensitivity and anxiety). The advantages over the use of single-item retrospective self-report are interesting in the research setting; at the same time, compliance evaluation may emerge as an important predictive value for a possible therapeutic outcome in the clinical setting. Within these premises, a smartphone-based EMA approach can be used to increase knowledge on several aspects of AB, even included the natural course and fluctuations of signs, symptoms, and exposure to etiological factors.
You have the opportunity to gather more in-depth information about bruxism assessment in our course "Encyclopedia of Bruxism and Apnea" by Sadao Sato, Carlo Poggio and other experts.
CONCLUSION
Within the limits of the present investigation, which was designed to assess for the first time the level of individual compliance with a smartphone-based EMA approach to the assessment of awake bruxism, findings suggest that such a strategy has interesting potential to collect data on AB for both clinical and research purposes. The mean compliance per day (i.e., percentage of alerts to which the subjects responded) was 67.8 ± 11.3% (range 44.5–91.4%) of the total alerts, and using the threshold of 60% responded alerts/day required less than 3 extra days to reach the minimum requirement of 7 days with a minimum of 12 answered alerts/day. These data might be used to standardize future reports for comparison purposes.
References
Lobbezoo F, Ahlberg J, Glaros AG, Kato T, Koyano K, Lavigne GJ et al (2013) Bruxism defined and graded: an international consensus. J Oral Rehabil 40:2–4.
Lobbezoo F, Ahlberg J, Raphael KG, Wetselaar P, Glaros A, Kato T et al (2018) International consensus on the assessment of bruxism: report of a work in progress. J Oral Rehabil 45:837–844.
Manfredini D, Restrepo C, Diaz-Serrano K, Winocur E, Lobbezoo F (2013) Prevalence of sleep bruxism in children: a systematic review of the literature. J Oral Rehabil 40:631–642.
Manfredini D, Winocur E, Guarda_Nardini L, Paesani D, Lobbezoo F (2013) Epidemiology of bruxism in adults: a systematic review of literature. J Orofac Pain 27:99–110.
Manfredini D, Bracci A, Djukic G (2016) BruxApp: the ecological momentary assessment of awake bruxism. Minerva Stomatol 65: 252–255
Bracci A, Djukic G, Favero L, Salmaso L, Guarda-Nardini L, Manfredini D (2018) Frequency of awake bruxism behaviors in the natural environment. A seven day, multiple-point observation of real time report in healthy young adults. J Oral Rehabil 45:423–429.
Zani A, Lobbezoo F, Bracci A, Ahlberg J, Manfredini D (2019) Ecological Momentary Assessment and Intervention principles for the study of awake bruxism behaviors, part 1: general principles and preliminary data on healthy young Italian adults. Front Neurol 10:169.
Osiewicz MA, Lobbezoo F, Bracci A, Ahlberg J, Pytko-PolonczyK J, Manfredini D (2019) Ecological Momentary Assessment and Intervention Principles for the study of awake bruxism behaviors, part 2: development of a smartphone application for a multicenter investigation and chronological translation for the Polish version. Front Neurol 10:170.
Runyan JD, Steinke EG (2015) Virtues, ecological momentary assessment/intervention and smartphone technology. Front Psychol 6:481.
Schiffman E, Ohrbach R, Truelove E, Look J, Anderson G, Goulet JP, List T et al (2014) Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group. J Oral Facial Pain Headache 28:6–27.
Stone AA, Shiffman S (1999) Ecological momentary assessment (EMA) in behavioral medicine. Ann Behav Med 16:199–202.
Hufford M (2007) Special methodological challenges and opportunities in ecological momentary assessment. In: Stone A, Schiffman S, Atienzae A, Nebeling L (eds) The science of real-time data capture: self-reports in health research. Oxford University Press pp, New York, pp 54–75
Raento M, Oulasvirta A, Eagle N (2009) Smartphones: an emerging tool for social scientist. Sociol Methods Res 37:426–454.
Runjan JD, Steenbergh TA, Bainbridge C, Daugherty DA, Oke L, Fry BN (2013) A smartphone ecological momentary assessment/intervention Bapp^ for collecting real-time data and promoting self-awareness. PLoS ONE 8:e71325.
Tsomos G, Ludwig B, Grossen J, Pazera P, Gkantidis N (2014) Objective assessment of patient compliance with removable orthodontic appliances. A cross-sectional cohort study. Angle Orthod 84: 56–61.
Charavet C, Le Gall M, Albert A, Bruwier A, Leroy S (2019) Patient compliance and orthodontic treatment efficacy of Planas functional appliances with TheraMon microsensors. Angle Orthod 89:117–122.
Schoot TC, Schlipf C, Glasl B, Schwarzer CL, Weber J, Ludwig B (2013) Quantification of patient compliance with Hawley retainers and removable functional appliances during the retention phase. Am J Orthod Dentofac Orthop 144:533–540.
Arreghini A, Trigila S, Lombardo L, Siciliani G (2017) Objective assessment of compliance with intra- and extraoral removable appliances. Angle Orthod 87:88–95.
Klaus K, Stark P, Serbesis TSP, Pancherz H, Ruf S (2017) Excellent versus unacceptable orthodontic results: influencing factors. Eur J Orthod 39:615–621.
Bertoldi C, Coming M, Guaraldi G, Ialla M, Guaitolini S, Generals L, Monzani D, Cortellini P, Zaffe D (2018) Are periodontal outcomes affected by personality patterns? A 18-month follow-up. Acta Odontol Scand 76:48–57.