Templates Cirúrgicos Protéticos e Preparação do Local de Implante Dentário: Um Estudo In Vitro
Tradução automática
O artigo original está escrito em EN language (link para lê-lo) .
Resumo
Numerosos tipos de guias cirúrgicos prostodônticos, com e sem mangas metálicas, mostraram-se úteis em estudos clínicos. O objetivo desta pesquisa in vitro foi comparar o tempo necessário para completar o procedimento cirúrgico com dois modelos de templates prostéticos cirúrgicos de design diferente. Dez modelos protótipos idênticos de mandíbula, baseados em uma CBCT e escaneamento óptico de um paciente parcialmente edêntulo com dentes ausentes nos números 37, 46 e 47, foram preparados e, em seguida, impressos. Cinco desses modelos foram utilizados para a preparação do local do implante com um guia cirúrgico sem mangas metálicas e um kit cirúrgico dedicado, e os outros cinco modelos foram utilizados para o mesmo procedimento realizado com um guia cirúrgico com mangas metálicas e um kit cirúrgico dedicado. O tempo de preparação do local do implante foi medido e registrado. A análise estatística foi realizada utilizando o teste t de Student para amostras independentes. Diferenças entre os grupos foram consideradas estatisticamente significativas (t = −9.94; df = 28; p = 0.0000) com um valor mais baixo a favor dos templates cirúrgicos sem mangas metálicas. Diferentes tipos de guias cirúrgicos prostodônticos, com ou sem mangas metálicas, parecem ser um fator importante que pode impactar significativamente o tempo de preparação do local do implante e, portanto, o procedimento cirúrgico geral.
Introdução
A implantologia dentária é um ramo da odontologia que visa restaurar dentes ausentes através da inserção de parafusos aloplásticos (de diferentes materiais) na estrutura óssea (implantes dentários). Basicamente, a implantologia é um procedimento de reabilitação destinado àqueles que perderam seus dentes naturais. Dentes artificiais são projetados para substituir dentes reais que estão ausentes em termos de estética e função mastigatória.
As técnicas de implantologia dentária de ponta permitem uma reabilitação permanente da mastigação e, nos últimos anos, têm se concentrado em melhorar os resultados estéticos. A previsibilidade dessas reabilitações está se tornando cada vez mais alta, especialmente devido à introdução da odontologia digital. Graças ao advento das tecnologias digitais, é possível programar, diagnosticar e planejar um tratamento com um fluxo de trabalho completamente digital.
A implantologia guiada é uma técnica moderna para posicionar implantes dentários em pacientes que sofrem de edentulismo (falta de um ou mais dentes) ou que passaram por uma extração dentária. Usando software, a cavidade oral do paciente é escaneada, criando um modelo 3D no qual o dentista pode planejar a cirurgia e visualizá-la. A principal vantagem dessa técnica é que ela permite que a cirurgia seja realizada exatamente como foi programada no computador, melhorando assim o desempenho mecânico e, portanto, a previsibilidade. O primeiro passo é realizar um exame oral do paciente; a cavidade oral é escaneada usando uma tomografia computadorizada 3D para montar o modelo digital da dentição. O exame radiográfico captura informações cruciais, como a posição dos nervos sensoriais, a posição do seio maxilar e outros pontos anatômicos de referência.
Essa simulação é então enviada para centros especializados que criam um “guia cirúrgico” usado para realizar a cirurgia sem afetar a gengiva; o parafuso é posicionado dentro dos tecidos e, consequentemente, na coroa dental visível. Graças ao planejamento preciso que ocorre antes da intervenção, o procedimento é concluído rapidamente. A literatura científica recente, incluindo estudos in vitro, revisões sistemáticas, ensaios clínicos multicêntricos e ensaios controlados randomizados, leva à conclusão de que o uso de guias cirúrgicos personalizados, CAD/CAM (projeto assistido por computador/manufatura assistida por computador) deve ser considerado o padrão ouro para alcançar alta precisão de implante, de acordo com um plano de tratamento orientado prosteticamente. Guias cirúrgicos estereolitográficos também são uma das aplicações mais populares da impressão 3D em cirurgia oral e maxilofacial. D’Souza dividiu os guias de implante em (a) não limitantes, (b) parcialmente limitantes e (c) completamente limitantes, de acordo com a quantidade de restrição cirúrgica oferecida pelos modelos de guia cirúrgico. Dentro desses, o grupo de design completamente limitante é o mais avançado e preciso, e pode ser dividido em três subgrupos: (c1) guias com mangas metálicas principais, (c2) guias sem mangas metálicas, apenas com plástico, e (c3) guias de plástico ou metal com estrutura aberta. A maioria dos estudos se concentrou na precisão da cirurgia guiada usando diferentes designs de modelos, concluindo que os modelos cirúrgicos sem mangas metálicas são mais precisos do que aqueles onde as mangas metálicas estão unidas. Além disso, alguns estudos também relataram que o tempo de cirurgia utilizado para a colocação guiada de implantes é mais curto em comparação com a abordagem manual. Por outro lado, outros estudos mostraram várias limitações da abordagem guiada. No entanto, não há estudos comparando o tempo de cirurgia com diferentes designs de modelos cirúrgicos.
O objetivo deste estudo in vitro foi comparar o tempo total utilizado para preparar os locais de implante usando dois guias cirúrgicos e kits cirúrgicos diferentes, dedicados aos mesmos implantes cônicos (TSIII, Osstem Implant, Seul, Coreia do Sul ®), mas com diferentes designs de template: guia plástico com e sem mangas metálicas. A hipótese nula era que não há diferença de tempo entre os dois protocolos diferentes.
Resultados
No total, 10 templates cirúrgicos foram impressos e, em seguida, utilizados para o presente estudo. Os modelos foram divididos aleatoriamente em dois grupos de cinco modelos cada. Três implantes de 4,0 mm de diâmetro e 10 mm de comprimento foram planejados nas posições 37, 46 e 47. Um total de 30 locais de implante foram preparados: 15 locais em cinco modelos usando o One Guide Kit ® (Osstem Implant, Seul, Coreia do Sul 2016 ®) (OGK) e 15 locais nos outros cinco modelos usando o Guide Kit Taper ® (Osstem Implant, Seul, Coreia do Sul 2010 ®) (GKT).
A Tabela 1 apresenta os resultados da análise estatística. O tempo médio no grupo de teste (sem mangas metálicas, OGK) foi de 99,63 ± 31,91 s, e no grupo controle (com mangas metálicas, e GKT) foi de 207,81 ± 27,53 s.
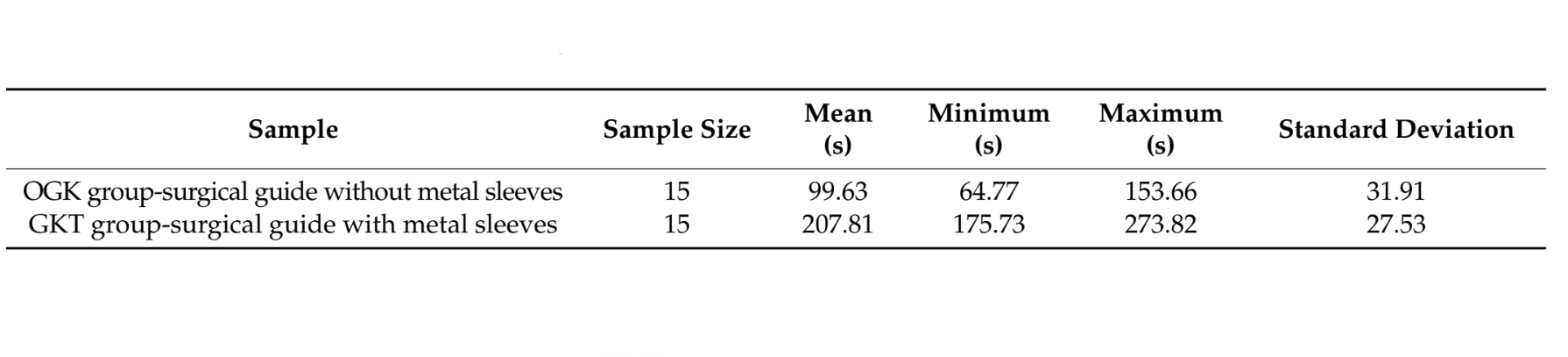
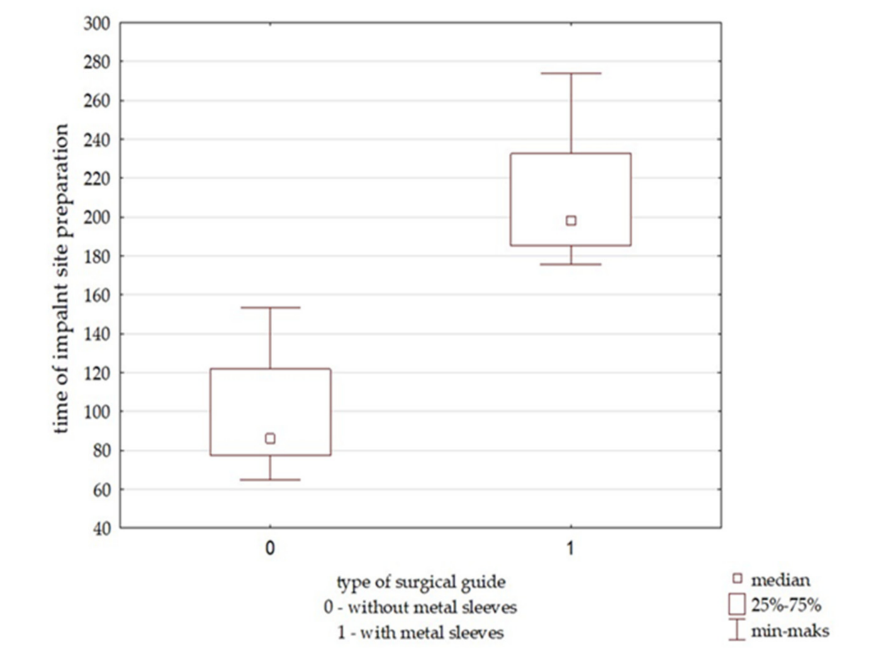
A diferença estatisticamente significativa entre o grupo teste e o grupo controle foi verificada com o teste estatístico t de Student. O valor de t do teste foi −9,94 com 28 graus de liberdade. O valor de p foi inferior a 0,05 (p = 0,000), provando que o tempo de preparação foi estatisticamente significativamente menor no grupo OGK do que no grupo GKT. A Figura 1 mostra as diferenças em termos do tempo de preparação do local do implante nos dois grupos.
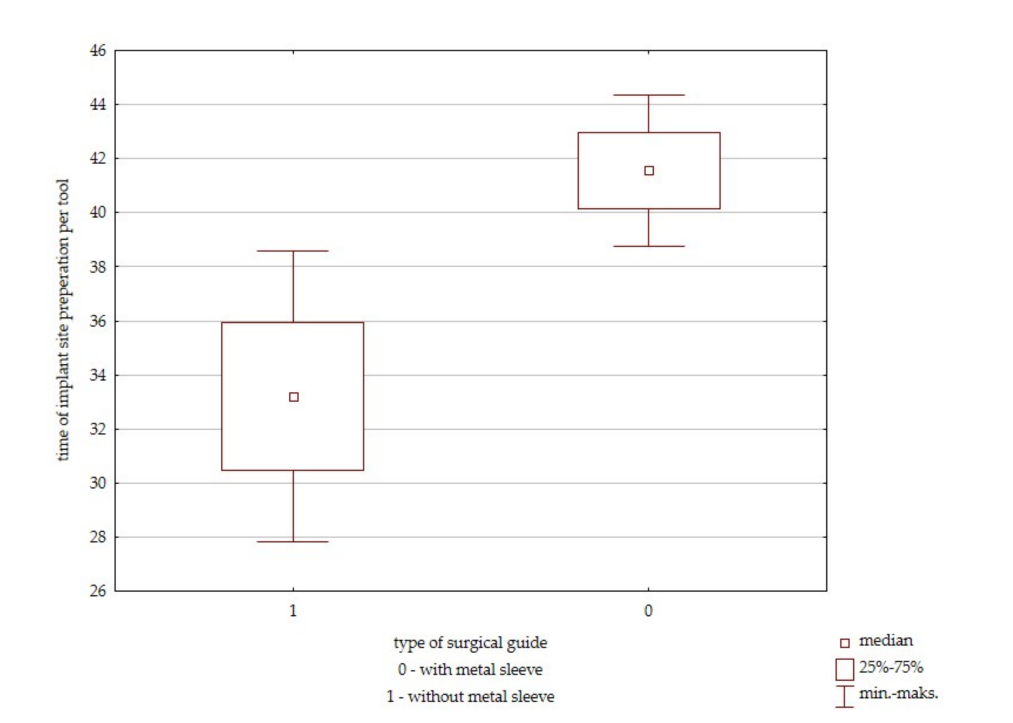
A diferença no tempo por ferramenta para cada grupo também foi verificada com o teste t de Student. O tempo médio de uso de cada ferramenta foi calculado em ambos os grupos, e os dados foram analisados. O valor t do teste foi −2,70 com 28 graus de liberdade. O valor p de Rafael Delgado-Ruiz foi inferior a 0,05 (p= 0,011), provando que o tempo de preparação por ferramenta também foi estatisticamente significativamente menor no grupo OGK do que no grupo GKT. A comparação é apresentada como boxplots (Figura 2).
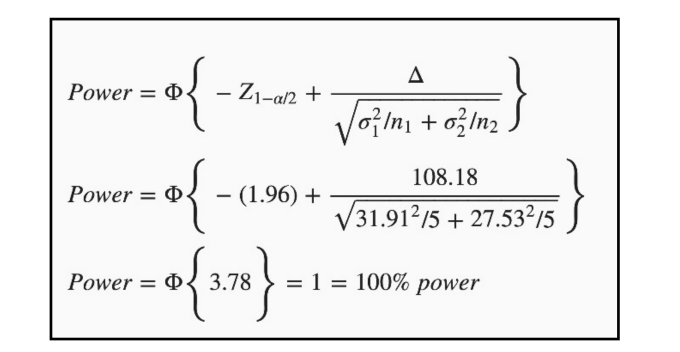
A análise dos boxplots demonstrou uma diferença estatisticamente significativa entre os grupos. Um cálculo de poder pós-hoc foi realizado para avaliar o poder estatístico do estudo. Dadas as médias dos pontos finais e o número de sujeitos, com alfa definido em 0,05, o poder pós-hoc foi de 100% (Figura 3).
Discussão
Este estudo focou no tempo necessário para a preparação do local do implante usando dois modelos cirúrgicos diferentes e os respectivos kits cirúrgicos dedicados. Dentro da pesquisa atual, cada local de implante foi preparado nas mesmas condições (37, 46, 47), de modo que apenas diferenças nas ferramentas cirúrgicas poderiam influenciar o tempo de preparação do local. Os resultados mostraram que a preparação do local do implante foi significativamente mais curta usando um modelo cirúrgico sem mangas metálicas e OGK. Com base nisso, a hipótese nula de que não há diferença foi rejeitada. Apesar do pequeno tamanho da amostra e da natureza in vitro do presente estudo, o desvio padrão foi semelhante em ambos os grupos, o que prova que as diferenças intragrupos eram semelhantes. Esse fator contribuiu para um poder pós-hoc muito alto do presente estudo. Os pesquisadores descobriram que o design de brocas cônicas com uma parte guia lisa em OGK permite usar cada diâmetro de broca, bem como diferentes componentes incluídos no kit, com a mesma parte de rastreamento de diâmetro fornecida pelo modelo de plástico impresso. As brocas GKT são cilíndricas, com algumas tendo uma parte guia lisa ajustada à manga metálica principal e outras não. Isso induz à necessidade de usar mangas metálicas removíveis adicionais para reduzir o diâmetro da manga guia principal para cada broca particular na sequência. Isso cria a necessidade de usar mais ferramentas (broca + manga de redução) ao trabalhar com GKT.
Na pesquisa atual, ocorreu um erro ao escolher as ferramentas apropriadas do kit GKT, enquanto não houve erros com o OGK.
O protocolo mais fácil de preparação do local do implante com design de guia sem mangueiras e OGK resulta em um menor risco de erro do operador, o que pode aumentar a segurança dos procedimentos cirúrgicos. O número reduzido de ferramentas cirúrgicas não apenas diminui o tempo durante a parte de perfuração da cirurgia, mas também pode reduzir o risco de erros do operador ou assistente e, assim, o risco total da cirurgia.
Casetta et al. descobriram que o espaço entre as brocas e as mangueiras metálicas incorporadas em templates plásticos ou mesmo o espaço entre as brocas e as mangueiras de redução podem levar a imprecisões durante a cirurgia. A precisão de dois designs e kits de guias cirúrgicas (OGK e GKT) foi comparada em um RCT com 100 implantes colocados. Dentro deste estudo, comparamos apenas o tempo de preparação do local do implante usando exatamente o mesmo kit e design de template. Um total de 41 implantes foram colocados com GKT e mangueiras metálicas incorporadas em um quadro de guia plástico, enquanto 49 implantes foram colocados com OGK com um quadro de guia plástico apenas. Templates cirúrgicos sem mangueiras metálicas foram considerados mais precisos em termos de plano vertical e ângulo em comparação com o template convencional com mangueiras metálicas. Comparando os requisitos para a preparação de ambos os kits, os investigadores notaram que incorporar uma mangueira metálica em um quadro impresso em 3D exigia 1 mm a mais de espaço interdentário para projetar o guia. Embora isso não tenha afetado nosso experimento planejado em locais molares, poderia ter limitações clínicas quando o espaço interdentário disponível é limitado, por exemplo, em pré-molares ou incisivos inferiores.
Além dos requisitos de espaço adicionais, Cassetta et al. descobriram que colocar uma manga metálica pré-fabricada dentro do template pode induzir erros durante a fabricação de um guia cirúrgico e, como mencionado anteriormente, as margens de folga entre a manga principal e a manga de redução para uma broca específica e entre a manga de redução e a broca podem resultar em imprecisões durante a cirurgia. Outro problema é o custo extra das mangas metálicas dedicadas, bem como o trabalho de laboratório para colocá-las e fixá-las com precisão no quadro do guia. Todos esses fatores aumentam o custo do tratamento, especialmente em casos onde vários implantes estão planejados. Portanto, guias cirúrgicos impressos em três dimensões com mangas não metálicas embutidas de diâmetro menor foram sugeridos por Schneider et al. para reduzir o movimento lateral da broca e a tolerância do instrumento, bem como o custo. Além disso, quando um quadro de guia impresso em 3D feito apenas de plástico é usado como um template cirúrgico, o dispositivo e a tecnologia de impressão 3D utilizada para a fabricação também podem ser pontos-chave para a precisão. Outra vantagem de um template impresso em 3D sem uma manga metálica é a possibilidade de projetar uma abertura bucal para facilitar a perfuração na região posterior (abertura bucal limitada). No entanto, as chamadas mangas abertas laterais mostraram fornecer menor precisão em comparação com mangas plásticas fechadas em templates impressos, mas maior precisão em comparação com procedimentos de implantação à mão livre. Por outro lado, mangas abertas laterais sem elementos metálicos incorporados podem ser o único design possível em algumas situações clínicas devido a limitações anatômicas, incluindo abertura bucal e espaço interdental.
Colombo et al., em uma revisão crítica baseada em ensaios clínicos randomizados sobre aplicações clínicas e a eficácia da cirurgia de implante guiada, concluíram que reduções no tempo cirúrgico e na dor pós-operatória são discutidas durante as cirurgias de implante guiadas. É importante mencionar que o estudo foi baseado em dois ECRs e, em ambos os casos, guias de implante estabilizados por osso ou tecido mole foram utilizados, o que significa que os pacientes passaram por intervenções cirúrgicas extensas. Em outro ECR, foi encontrado maior dor e inchaço pós-operatório em locais tratados à mão livre em comparação com aqueles com uma abordagem guiada. A diferença na experiência pós-operatória dos pacientes nesses estudos pode ser baseada na extensão da cirurgia em si. Em geral, a cirurgia em que o retalho extenso é elevado e um guia é posicionado na superfície óssea é mais traumática do que a colocação guiada com retalho mini ou sem retalho de implantes únicos ou múltiplos com um guia suportado por dente. Assim, pode não haver diferença significativa para o paciente se a cirurgia extensa for realizada de forma guiada ou à mão livre, enquanto pode haver diferenças significativas para cirurgias menos extensas. Além disso, a precisão da colocação de implantes guiados varia dependendo se é uma cirurgia simples ou complexa. O mesmo tempo necessário para a estabilização precisa do guia com âncoras ósseas durante a cirurgia extensa pode desaparecer ao comparar o tempo necessário para realizar uma cirurgia semelhante à mão livre sem esse processo. No entanto, os tempos de cirurgia principal e preparação dos locais de implante podem ser mais curtos com uma abordagem guiada ou mesmo se dispositivos de guia simples forem utilizados. Analisando fatores de risco para complicações pós-operatórias após cirurgia oral, Shigeishi et al. encontraram que a duração prolongada da operação é um fator de risco significativo em pacientes que se submeteram a cirurgia oral.
Considerando que diferentes cirurgias requerem diferentes tempos para a preparação do campo operatório, anestesia, reflexões de retalho e instalação e fixação de moldes, uma abordagem guiada proporciona maior precisão durante os procedimentos de implante.
Houve limitações neste estudo. A comparação de precisão entre guias e kits testados foi impossível de realizar dentro do ensaio in vitro. Essa limitação foi baseada nas propriedades do material do modelo do estudo. Como o local do implante realizado no modelo de plástico rígido, de acordo com a recomendação do fabricante para osso duro, é menor em diâmetro do que a rosca do implante, e como a resistência do poliamida é muito alta, é impossível colocar um implante com o torque apropriado. Durante a colocação do implante, o torque aplicado levou à destruição imediata do design de transferência do implante a ser utilizado durante a colocação guiada do implante. Portanto, para comparar com precisão dois designs de molde idênticos e kits cirúrgicos no RCT, decidiu-se focar apenas na comparação de tempo dentro deste estudo in vitro. Outra limitação é que o tempo de perfuração dentro do osso nativo pode diferir da perfuração em modelos plásticos. No entanto, dependendo do tipo de osso ou sua dureza, os procedimentos de perfuração em diferentes locais ou em diferentes pacientes podem levar diferentes quantidades de tempo. É quase certo que a quantidade absoluta de tempo necessária para a preparação do local no osso pode ser diferente daquela em modelos plásticos. No entanto, os resultados deste estudo sugerem que o uso de um guia sem mangueira com OGK pode reduzir significativamente o tempo de preparação do local do implante em comparação com um guia de mangueira e GKT dedicado. Isso pode ser especialmente importante se múltiplos implantes forem colocados durante a cirurgia.
Além de todos os aspectos intra-cirúrgicos das terapias de implante baseadas em templates, esses procedimentos são precedidos por um cuidadoso processo diagnóstico. Uma fase de planejamento com o uso de imagens de CBCT, escaneamentos de tecidos orais e visualização do plano de restauração final pode ser útil durante a comunicação entre paciente e médico. Compreender o plano de tratamento e todos os seus benefícios, incluindo menor invasividade, menos dor, melhor precisão e, como indicado neste estudo, menor tempo cirúrgico com terapia de implante suportada digitalmente, pode ser benéfico para reduzir o medo e a ansiedade entre os pacientes.
Materiais e Métodos
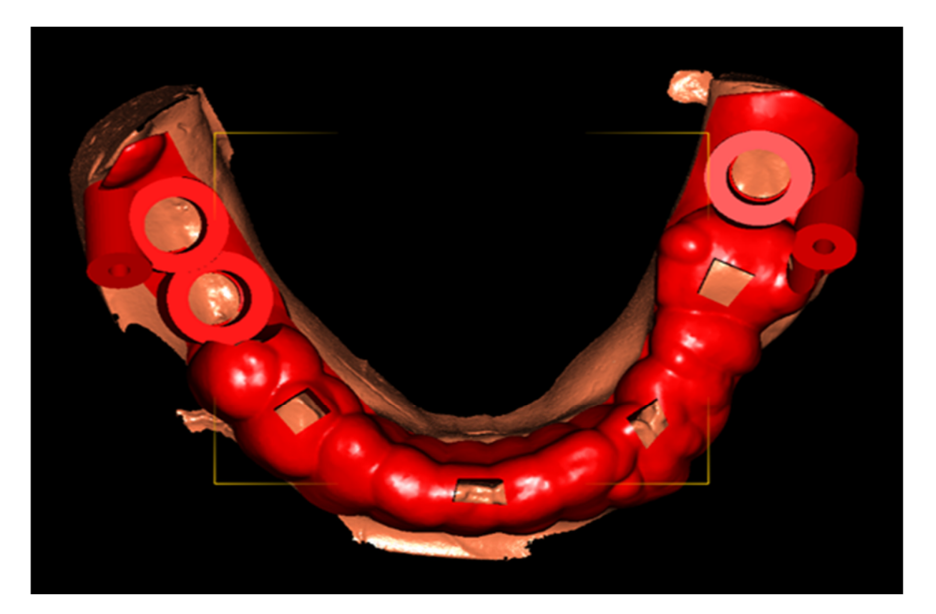
Modelos para o experimento foram criados com base em dados previamente coletados de um homem parcialmente edêntulo de 56 anos, com dentes faltando números 37, 46 e 47. Os dados DICOM (Digital Imaging and Communications in Medicine) do paciente foram derivados de uma varredura anterior de CBCT (tomografia computadorizada de feixe cônico, NewTom 5G XL, CEFLA s.c., Imola, Itália). O modelo de gesso armazenado representando a anatomia dos tecidos duros e moles foi digitalizado com um scanner de laboratório (Ceramill Map 600, Amann Girrbach AG, Koblach, Áustria), e os dados foram importados para o software DDS-Pro (JST, Częstochowa, Polônia). O modelo digitalizado foi salvo como um arquivo STL (Standard Triangulation Language) e, em seguida, impresso usando a tecnologia SLS (Selective Laser Sintering) e material em pó de poliamida (SL01, Sondasys, Ogrodzieniec, Polônia). Um centro de impressão externo preparou todos os modelos (Sondasys, Ogrodzieniec, Polônia). A Figura 4 mostra o modelo impresso em 3D.

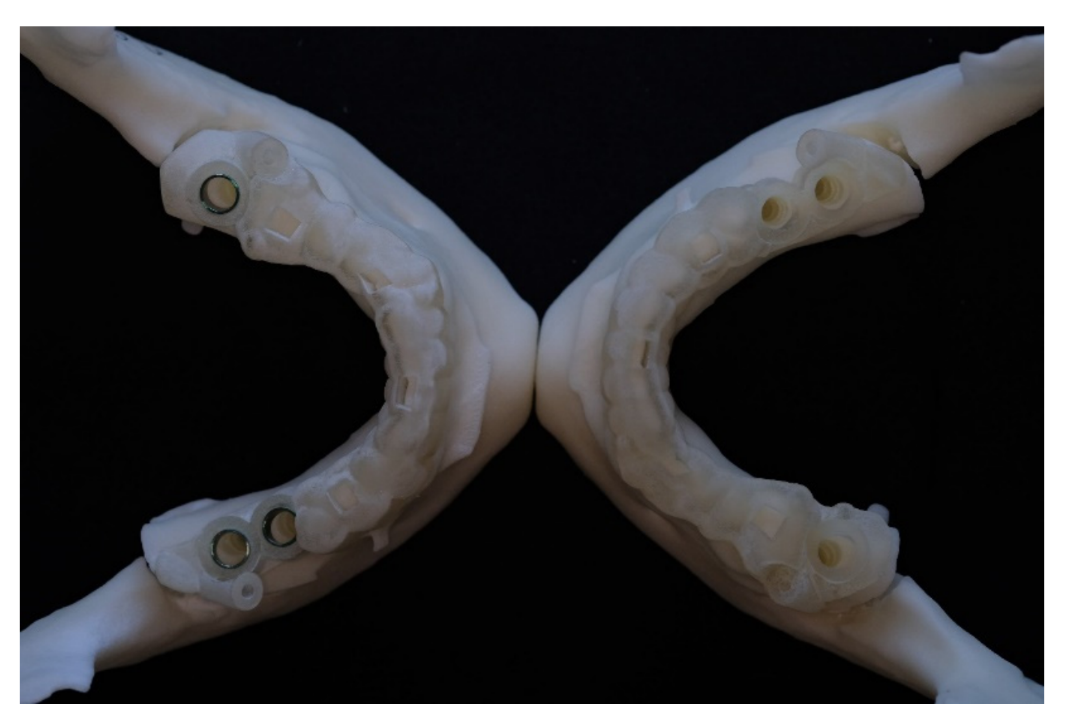
O software DDS-Pro foi utilizado para planejar virtualmente implantes de 4,0 mm de diâmetro e 10 mm de comprimento, nas posições corretas, guiadas prosteticamente. Dois tipos de guias cirúrgicas (Figura 5) foram projetadas de acordo com as recomendações do fabricante, para serem usadas com dois kits cirúrgicos diferentes, para a colocação dos mesmos implantes cônicos (Implantes TSIII SA, Osstem Implants, Seul, Coreia do Sul). Um template cirúrgico sem mangas metálicas foi projetado para ser utilizado com o novo Kit OneGuide (Grupo de teste, OGK, Osstem Implants), enquanto um segundo template cirúrgico foi preparado para incorporar mangas metálicas dedicadas a implantes de 4,0 mm de diâmetro (Manga metálica verde, Osstem Implants) com o Kit Taper (Grupo controle, GKT, Osstem Implants).
Os guias foram projetados na mesma forma, de modo que a única diferença entre eles era o diâmetro dos furos, preparados de acordo com os diferentes requisitos do kit cirúrgico (Figuras 6 e 7). O GKT exigia 1 mm a mais para incorporar e colar a manga metálica dedicada ao guia cirúrgico. Ambos os modelos foram impressos em 3D em um centro de impressão externo (Natrodent, Łódź, Polônia) usando tecnologia de múltiplos jatos (MP3000, 3D Systems, material: suportes S100, guia MP100, 3D Systems, Rock Hill, SC, EUA). Após a impressão, os modelos cirúrgicos foram colocados em um congelador por alguns minutos. Isso permitiu a fácil remoção das impressões da placa de construção da impressora. Uma vez que os modelos cirúrgicos foram removidos da placa de construção, o material de suporte foi removido em um forno de convecção a 70°C por 30 min. Depois disso, qualquer material de suporte restante foi removido com uma toalha de papel e um banho ultrassônico a aproximadamente 65°C (5 min). Finalmente, os modelos cirúrgicos foram enxaguados com água morna e sabão e secos com uma toalha de papel e ar comprimido seco. Após a verificação, os modelos cirúrgicos foram enviados para o teste in vitro.

Todos os modelos foram divididos aleatoriamente em dois grupos. O primeiro grupo envolveu o uso de um guia com mangas metálicas e o GKT, enquanto, no segundo grupo, os templates cirúrgicos foram produzidos sem mangas metálicas, para serem usados com o OGK.
Três locais de implante foram preparados em cada modelo de estudo, de acordo com o plano virtual e as instruções do fabricante. Os procedimentos de perfuração foram realizados pelo mesmo operador especialista com ambos os kits cirúrgicos (Ł.Z.), utilizando o dispositivo cirúrgico Implantmed (W&H Dentalwerk Bürmoos GmbH, Bürmoos, Áustria) com uma velocidade de 1200 rpm e torque máximo sob irrigação com solução salina fria.
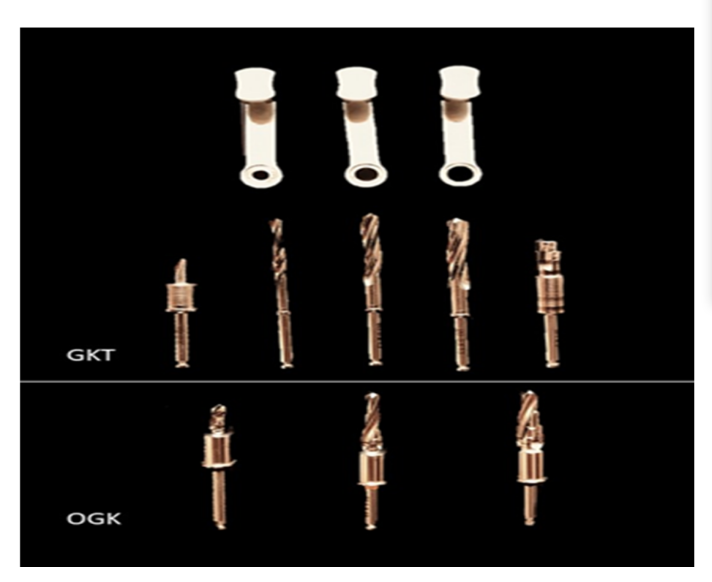
As medições de tempo foram feitas com um cronômetro digital (iPhone 8, Apple Inc., Cupertino, CA, EUA). O período de tempo começou após a colocação do template cirúrgico e terminou ao remover a última broca. As medições de tempo foram registradas em minutos, segundos e centésimos de segundo, e foram relatadas no software Excel (Microsoft Corporation, Redmond, Washington, DC, EUA) pelo mesmo avaliador de resultados (M.C.). Os tempos medidos incluíram o tempo necessário para trocar as brocas, e foram registrados, independentemente, para cada local de implante. Todas as ferramentas foram armazenadas no kit e verificadas antes de cada procedimento de preparação do local. O protocolo de perfuração necessário para a preparação do local do implante (por exemplo, diâmetro de 4,0 mm e comprimento de 10 mm) foi conforme sugerido pelo fabricante. No entanto, não era igual em ambos os kits cirúrgicos. Para os guias cirúrgicos sem mangas (OGK), apenas três brocas cirúrgicas foram utilizadas, enquanto, com o kit que requer mangas metálicas (GKT), cinco brocas cirúrgicas e três reduções metálicas (chaves) foram necessárias para preparar o local (Figura 8).
A comparação do tempo de preparação foi analisada usando o teste t de Student para amostras independentes (Statistica, StatSoft Polska, Cracóvia, Polônia). Um valor de p < 0,05 foi considerado estatisticamente significativo. Os resultados são apresentados como a média ± desvio padrão, e intervalos de confiança clássicos de 95% foram calculados.
Conclusões
Levando em consideração os resultados deste estudo com todas as suas limitações, podemos concluir que, utilizando um guia impresso em 3D feito apenas de plástico com um OGK dedicado, requer-se menos tempo para preparar o local do implante em comparação ao uso de um guia de plástico com uma manga metálica incorporada e um conjunto cirúrgico GKT dedicado. As mangas metálicas podem ser consideradas uma ajuda segura para a cirurgia oral. Portanto, as estruturas anatômicas não são danificadas pela sua aplicação. O tempo de cirurgia mais curto ao usar um guia impresso em 3D feito apenas de plástico se torna outro fator clinicamente valioso, além da maior precisão e menores custos de produção quando comparado a templates tradicionais com mangas metálicas. Houve muitas mudanças na tecnologia desde 1992, quando começou a era da implantologia digital. Com as melhorias na tecnologia de impressão 3D e mudanças no design de brocas guiadas (de cilíndricas que requerem mangas metálicas incorporadas ao template para proteger a parte de plástico do guia durante a perfuração, para brocas cônicas com uma parte de guia lisa unificada), podemos observar a evolução da implantologia digital. Menor custo, maior precisão e cirurgias mais curtas são os fatores mais importantes apreciados pelos clínicos, assim como pelos pacientes.
Łukasz Zadrożny, Marta Czajkowska, Marco Tallarico, Leopold Wagner, Jarosław Markowski, Eitan Mijiritsky e Marco Cicciù
Referências
- Mumoli, N.; Busoni, A.; Cei, M. Uma prótese dentária engolida. Lancet 2009, 373, 1890.
- Bjertness, E.; Hansen, B.F.; Berseth, G.; Gronnesby, J.K. Higiene oral e periodontite em jovens adultos. Lancet 1993, 342, 1170–1171.
- Bramanti, E.; Norcia, A.; Cicciù, M.; Matacena, G.; Cervino, G.; Troiano, G.; Zhurakivska, K.; Laino, L. Implante dentário pós-extração na zona estética, técnica do escudo do alvéolo versus protocolo convencional. J. Craniofacial Surg. 2018, 29, 1037–1041.
- Lavorgna, L.; Cervino, G.; Fiorillo, L.; Di Leo, G.; Troiano, G.; Ortensi, M.; Galantucci, L.; Cicciù, M. Confiabilidade de um projeto prostodôntico virtual realizado através de uma aquisição fotográfica 2D e 3D: Um estudo experimental sobre a precisão de diferentes sistemas digitais. Int. J. Environ. Res. Public Health 2019, 16, 5139.
- Ortiz, C.; Boyce, M.C. Ciência dos materiais. Materiais estruturais bioinspirados. Science 2008, 319, 1053–1054.
- Laino, L.; Cicciù, M.; Fiorillo, L.; Crimi, S.; Bianchi, A.; Amoroso, G.; Monte, I.P.; Herford, A.S.; Cervino, G. Risco cirúrgico em pacientes com coagulopatias: Diretrizes para pacientes hemofílicos para cirurgia oro-maxilofacial. Int. J. Environ. Res. Public Health 2019, 16, 1386.
- Cicciù, M.; Fiorillo, L.; D’Amico, C.; Gambino, D.; Amantia, E.M.; Laino, L.; Crimi, S.; Campagna, P.; Bianchi, A.; Herford, A.S.; et al. Sistemas de Impressão Digital 3D Comparados com Técnicas Tradicionais em Odontologia: Uma Revisão Sistemática de Dados Recentes. Materials 2020, 13, 1982.
- Scrascia, R.; Fiorillo, L.; Gaita, V.; Secondo, L.; Nicita, F.; Cervino, G. Prótese Suportada por Implante para Reabilitação de Paciente Edêntulo. Da Prótese Temporária à Definitiva com um Novo Protocolo: Um Relato de Caso Único. Prosthesis 2020, 2, 10–24.
- Urban, I.; Caplanis, N.; Lozada, J.L. Regeneração óssea guiada vertical simultânea e regeneração tecidual guiada na maxila posterior usando fator de crescimento derivado de plaquetas humanas recombinante: Um relato de caso. J. Oral Implantol. 2009, 35, 251–256.
- Cicciù, M.; Cervino, G.; Terranova, A.; Risitano, G.; Raffaele, M.; Cucinotta, F.; Santonocito, D.; Fiorillo, L. Parâmetros Protéticos e Mecânicos do Osso Facial sob a Carga de Diferentes Formas de Implantes Dentários: Um Estudo Paramétrico. Prosthesis 2019, 1, 41–53.
- D’Amico, C.; Bocchieri, S.; Sambataro, S.; Surace, G.; Stumpo, C.; Fiorillo, L. Considerações sobre Carga Oclusal em Restaurações Fixas Suportadas por Implante. Prosthesis 2020, 2, 252–265.
- Tallarico, M.; Czajkowska, M.; Cicciù, M.; Giardina, F.; Minciarelli, A.; Zadroz˙ny, Ł.; Park, C.J.; Meloni, S.M. Precisão de templates cirúrgicos com e sem mangas metálicas em casos de restaurações de arco parcial: Uma revisão sistemática. J. Dent. 2021, 115, 103852.
- Park, J.Y.; Song, Y.W.; Park, S.H.; Kim, J.H.; Park, J.M.; Lee, J.S. Fatores clínicos que influenciam o posicionamento do implante por cirurgia guiada usando um template sem manga metálica na crista parcialmente edêntula: Análise de regressão múltipla de uma coorte prospectiva. Clin. Oral Implant. Res. 2020, 31, 1187–1198.
- Zadrożny, Ł.; Czajkowska, M.; Mijiritsky, E.; Wagner, L. Repetibilidade de Implantações à Mão Livre Suportadas com Mangas Plásticas Universais - Estudo In Vitro. Int. J. Environ. Res. Public Health 2020, 17, 4453.
- Tallarico, M.; Martinolli, M.; Kim, Y.; Cocchi, F.; Meloni, S.M.; Alushi, A.; Xhanari, E. Precisão da Colocação de Implantes Baseada em Template Assistido por Computador Usando Dois Diferentes Templates Cirúrgicos Projetados com ou sem Mangas Metálicas: Um Estudo Controlado Randomizado. Dent. J. 2019, 7, 41.
- Marlière, D.A.A.; Demètrio, M.S.; Picinini, L.S.; Oliveira, R.G.; Netto, H. Precisão da cirurgia guiada por computador para colocação de implantes dentários em pacientes totalmente edêntulos: Uma revisão sistemática. Eur. J. Dent. 2018, 12, 153–160.
- Tallarico, M.; Caneva, M.; Baldini, N.; Gatti, F.; Duvina, M.; Billi, M.; Iannello, G.; Piacentini, G.; Meloni, S.M.; Cicciù, M. Reabilitação centrada no paciente de edentulismo único, parcial e completo com prótese dentária fixa cimentada ou retida por parafuso: A Primeira Conferência de Consenso do Centro de Pesquisa e Educação em Implantes Dentários Avançados Osstem 2017. Eur. J. Dent. 2018, 12, 617–626.
- Tahmaseb, A.; Wu, V.; Wismeijer, D.; Coucke, W.; Evans, C. A precisão da cirurgia de implante assistida por computador estática: Uma revisão sistemática e meta-análise. Clin. Oral Implant. Res. 2018, 29 (Suppl. 16), 416–435.
- Van de Wiele, G.; Teughels, W.; Vercruyssen, M.; Coucke, W.; Temmerman, A.; Quirynen, M. A precisão da cirurgia guiada através de templates cirúrgicos estereolitográficos suportados por mucosa nas mãos de cirurgiões com pouca experiência. Clin. Oral. Implant. Res. 2015, 26, 1489–1494.
- Van Assche, N.; Vercruyssen, M.; Coucke, W.; Teughels, W.; Jacobs, R.; Quirynen, M. Precisão da colocação de implantes assistida por computador. Clin. Oral Implant. Res. 2012, 23 (Suppl. 6), 112–123.
- Javaid, M.; Haleem, A. Status atual e aplicações da fabricação aditiva na odontologia: Uma revisão baseada na literatura. J. Oral Biol. Craniofac. Res. 2019, 9, 179–185.
- Louvrier, A.; Marty, P.; Barrabé, A.; Euvrard, E.; Chatelain, B.; Weber, E.; Meyer, C. Quão útil é a impressão 3D na cirurgia maxilofacial? J. Stomatol. Oral Maxillofac. Surg. 2017, 118, 206–212.
- Tack, P.; Victor, J.; Gemmel, P.; Annemans, L. Técnicas de impressão 3D em um ambiente médico: Uma revisão sistemática da literatura. Biomed. Eng. Online 2016, 15, 115.
- Di Giacomo, G.; Silva, J.; Martines, R.; Ajzen, S. Guia cirúrgico de sinterização seletiva a laser projetado por computador e implantes dentários com carga imediata com prótese definitiva em paciente edêntulo: Um método preliminar. Eur. J. Dent. 2014, 8, 100–106.
- D’Souza, K.M.; Aras, M.A. Tipos de guias cirúrgicas de implante em odontologia: Uma revisão. J. Oral Implantol. 2012, 38, 643–652.